One code. One claim. One costly outcome.
In medical coding, while errors are rarely intentional, two of the most common pitfalls are upcoding and downcoding. They sit on opposite ends of the accuracy spectrum but create serious financial and regulatory exposure.
Let’s break down the key differences between upcoding and downcoding and outline best practices to ensure accurate reimbursement and compliance.
Upcoding occurs when a provider assigns a medical code that reflects a higher level of complexity, severity, or service than what was actually performed or supported by the clinical documentation. While some errors are unintentional, upcoding becomes a compliance concern when higher-level codes are deliberately used to maximize reimbursement from Medicare, Medicaid, or commercial payers.
Common upcoding examples include:
Upcoding errors often arise from a combination of process gaps, documentation challenges, and operational pressures, including:
Downcoding occurs when a provider assigns a lower-level code than what was actually performed or supported by the clinical documentation. It’s often driven by caution, such as concerns about audits or denials, but results in underbilling for care that was legitimately delivered. Over time, this approach erodes revenue and undervalues your work.
Common downcoding examples include:
Providers often downcode due to:
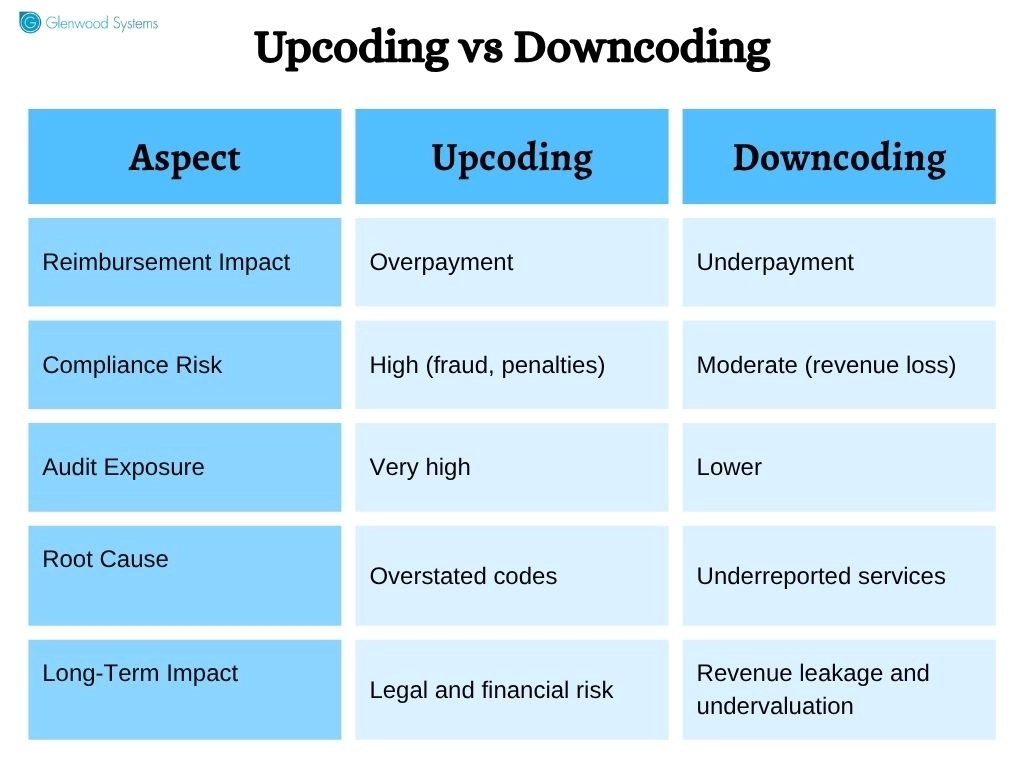
Upcoding vs Downcoding
Upcoding and downcoding may seem like opposite errors, but they disrupt the same goal: an accurate, defensible representation of care delivered. Here's how they impact your practice.
Revenue integrity is built on accuracy, and coding errors compromise that very foundation.
Upcoding may boost short-term overpayments, but can trigger audits, recoupments, penalties, and payer scrutiny. Downcoding, on the other hand, results in underbilling, leading to revenue leakage, lower case mix index (CMI), undervalued provider productivity, and reduced funding, especially in value-based payment models.
Accurate medical coding is an ethical responsibility that also impacts reimbursement and quality reporting.
Upcoding misinterprets the complexity of care delivered. Downcoding, while not inherently unethical, underreports the level of care delivered and fails to accurately reflect clinical effort, patient acuity, and medical decision-making. Both distort the true picture of care.
Upcoding poses the greatest legal risk, exposing organizations to allegations of fraud, civil penalties, False Claims Act liability, and heightened audit activity from payers. The False Claims Act penalty ranges from $14,308 to $28,619 per claim, in addition to treble damages. Even isolated coding issues can escalate into substantial financial and legal exposure.
Downcoding poses less direct legal exposure, but can raise concerns around data integrity, quality reporting, and risk adjustment accuracy.
Downcoding can understate patient complexity, resulting in lower risk scores, reduced value-based incentives, and inaccurate population health data.
Upcoding, on the other hand, inflates patient severity and risk scores, distorting performance metrics and reimbursement.
Over time, coding inaccuracies can result in:
Sustained revenue integrity relies on consistent, accurate coding practices. The following best practices will help you minimize coding errors and stay compliant.
Upcoding and downcoding differ in direction but lead to the same core issue.
The solution isn’t aggressive coding or overly conservative medical billing; it’s accurate, defensible coding that truly reflects the care delivered. At Glenwood Systems, our advanced AI scribe and automated coding solutions ensure comprehensive documentation and validate codes against payer requirements to protect revenue integrity.
Let's connect to explore how to improve coding accuracy without adding more work.
Schedule a Free Consultation!
